Cocaine Abuse
Cocaine is still the most abused stimulant. Many people, outside of the drug rehab field, have lost sight of cocaine as a major drug problem, but this is due to the fact that the news media isn’t covering the epidemic like it did in the 1980s when cocaine was being seen as the “disco drug” of the time.
Danger
The most current data that establishes this drug as being the highest used stimulant comes from information from emergency room visits where cocaine is a major part of the emergency.
The public has become apathetic about the dangers of cocaine, which is reflected in the ideas seen in the general public believing that cocaine is a safe recreational drug. This idea of cocaine being a recreational drug is exemplified in the slang names that are currently popular for cocaine. These are a few of those terms that are descriptive of an unreal description of cocaine: “status stimulant, yuppie drug, and Cadillac of stimulants”. Its most popular name, “coke” can make someone equate it with a cola drink rather than describing the dangerous effects that come from this, many times, lethal drug.
Most of the public believes that cocaine isn’t too dangerous because of the common false data that cocaine isn’t addictive. An earlier published article on “Cocaine Addiction Symptoms” dispels that myth. Cocaine is one of the most psychologically addictive drugs and there is ample evidence that shows how it is also physically addicting. Admittedly, cocaine’s physical withdrawals are not as severe, in the short term as alcohol or opiates, but there are many ways that continual use of cocaine changes certain physiological reactions that will cause a withdrawal syndrome if abruptly stopped after prolonged use.
Most of the current trends of using cocaine see it as an adjunct to getting high when combined with other drugs. It is common to see cocaine used with alcohol, sedatives, such as Xanax or as a “speedball” when it is combined with heroin. These depressant drugs are used to counteract the stimulant effects of cocaine which, when used alone, can be overpowering and cause an unwanted effects of dysphoria ( a state of unease or generalized dissatisfaction) or a feeling of depression in some and it produces anxiety attacks in others, but neither of these effects are pleasant and are not the product that drug seekers are trying to elicit.
In adolescents, we find that cocaine is combined with marijuana and/or alcohol to moderate the “speedy” effects of the drug.
Cocaine gives the user a feeling of power and omnipotence that is sought after by many who are very successful in their ambitious careers, making it a drug of choice for this segment of the population.

Origin
The cocaine that is sold on the streets in America commonly comes in the form of cocaine hydrochloride that is being produced in South America, especially in Colombia. This hydrochloride salt of cocaine is smuggled into New York and Los Angeles in a very pure form that is 90 to 95% pure cocaine.
It is then cut or diluted as it passes through the different “middlemen” that are part of the distribution system in the U.S.
The final cocaine product may be diluted to a form that has as little as 1% pure cocaine. Cocaine is commonly diluted with simple sugars, such as mannitol, lactose or glucose.
Compounding the drug effect and the intrinsic dangers of cocaine comes from some dealers that cut the cocaine with other drugs such as PCP, LSD or methamphetamines as well as local anesthetic drugs like procaine and lidocaine.
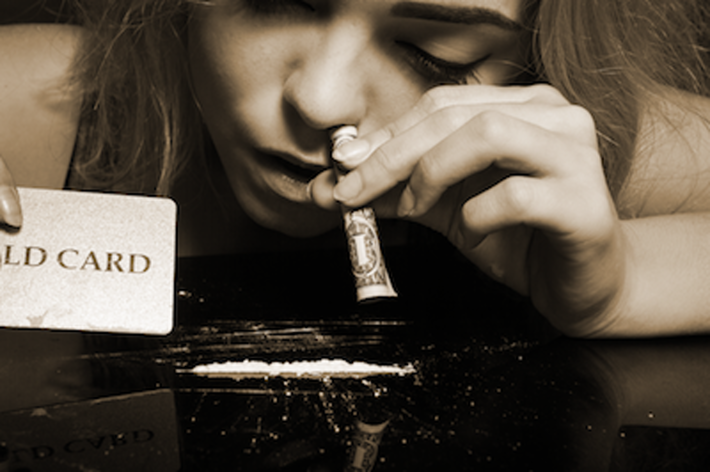
Cocaine users are seeking the euphoric high that comes with the drug’s initial stimulation of the Central Nervous System. This can be achieved by snorting the powder into one’s lungs, which is the common practice seen in movies where a user will take a rolled up dollar bill and use it as a straw to inhale a “line” of cocaine that is spread out on a hard surface.
It is also injected into one’s veins by dissolving the drug in water and then injecting it directly into the blood stream.
There is also a technique known as “freebasing” that converts cocaine hydrochloride into cocaine sulfate, which frees the cocaine of the additives and makes the vapors from burning the cocaine nearly 100% pure so the initial “blast” of cocaine reaching the brain gives the “jolt” that the cocaine user is seeking. Unfortunately, this process requires highly volatile solvents, like ether, which in the drug-impaired hands of a cocaine addict is lending itself to dangers of explosions and many cases of severe burns.
Crack Cocaine
The development of crack cocaine made this drug accessible to many that couldn’t afford the price of powdered cocaine. Crack is extracted from the cocaine using baking soda and heat. This method is much safer than “freebasing”. The product of this method is a crystalline rock of cocaine that can be sold in small quantities and is vaporized or smoked in a glass pipe over open flame. Many people describe crack cocaine’s effects as being ten times stronger than straight cocaine. The effects of crack wear off in a matter of minutes, causing the user to seek repeated smoking of these rocks until his body is so exhausted that he begins to feel the untoward effects of paranoia and elevated fear, rather than euphoria. This doesn’t stop a crack user from continuing to search for the original high that was so pleasurable.
In spite of the common wisdom that cocaine abuse is passé, there are many in our society who suffer from this addiction and require effective residential treatment. The holistic rehabilitation model of Narconon is a long-established, highly effective program for the treatment of cocaine addiction.
If you or someone you love needs help in getting off cocaine for good
call Narconon today

